Nous sommes ravis de vous aider et nous vous répondrons dès que possible.
Accédez à l'ensemble des documents, vidéos, articles, modules d'e-learning et autres ressources relatives à tous nos produits.




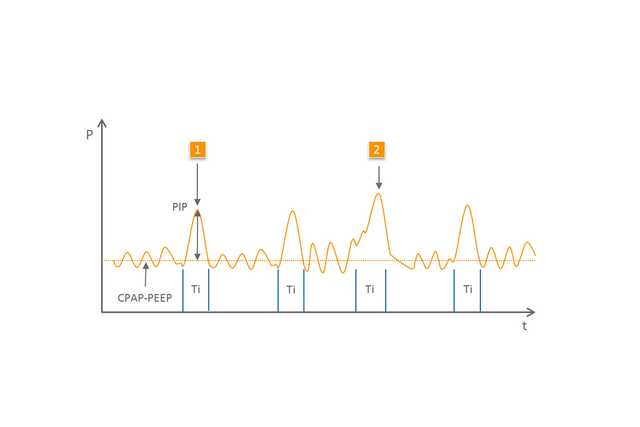
Le terme générique NIPPV inclut des modes dans lesquels – outre la CPAP/PEEP – des cycles respiratoires contrôlés sont appliqués pour aider le patient. Ces cycles respiratoires affichent un niveau de pression plus élevé et ne sont pas émis de manière synchronisée. Une différenciation est faite entre les divers variants de cette forme d'assistance respiratoire (
La thérapie NIPPV (
Assistance respiratoire contrôlée pour les nouveau-nés
Assistance efficace après extubation et pendant l'apnée (1,2)
Simple à utiliser et à ajuster
Disponible avec les dispositifs medinCNO, medinCNOmini, medin-NC3
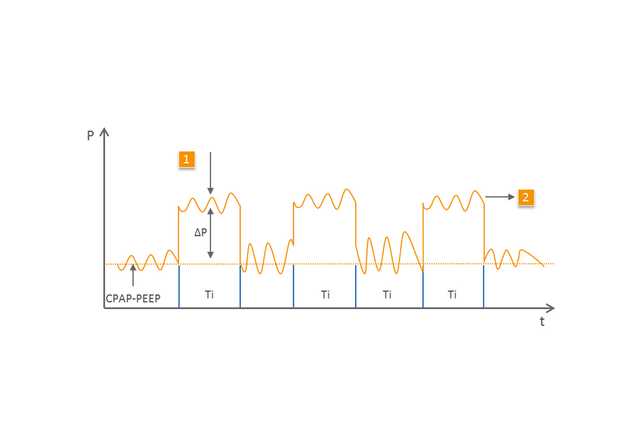
Le mode BiLevel (
1 Cycle mécanique
2 Cycle spontané au deuxième niveau de pression supérieure
Les effets et l'efficacité de la NIPPV ont été étudiés dans de nombreuses études (
Les dispositifs de CPAP spécialisés de medin utilisés avec le générateur de nCPAP Medijet sont parfaitement adaptés pour l'utilisation de la NIPPV et du mode BiLevel. Avec un débit de base, le patient reçoit la CPAP/PEEP souhaitée. Avec l'aide d'un deuxième niveau de débit qui est défini en plus du débit de base via un débitmètre électronique supplémentaire, Medijet génère un niveau de pression supérieur.
Puisque Medijet permet une expiration à tout moment, le patient peut respirer librement aux deux niveaux de pression. C'est pourquoi les dispositifs de CPAP medin permettent toutes les options d'assistance respiratoire par NIPPV.